In 2 of these studies, however, there were only about 20 patients randomized to each study arm, with even fewer completing the study.5,6 Another study did not have a control group and had an extremely high reinfection rate, suggesting that H pylori was not truly eradicated.4 Most importantly, none of these 3 studies had a true untreated, placebo group, and none provided data on an intention-to-treat basis. What are other possible causes for my stomach pain? For functional or non-ulcer dyspepsia, some basic questions to ask your doctor include: In addition to the questions that youve prepared to ask your doctor, dont hesitate to ask questions during your appointment at any time that you dont understand something. To determine whether H pylori infection causes nonulcer dyspepsia, we enrolled patients infected with H pylori, but without active ulcer disease, in a randomized, double-blind, placebo-controlled clinical trial. H. pylori. JRDunn
1999;159(19):22832288.
Furthermore, treatment of patients with nonulcer dyspepsia can be challenging because of the need to balance medical management strategies (e.g., eradication of Helicobacter pylori) with treatments for psychologic or functional disease. Addressing only one factor, such as H. pylori infection or motility dysfunction, is unlikely to be successful and may be frustrating for the patient and the physician. MKorman et al. JPArends
JPArends
By continuing to use our site, or clicking "Continue," you are agreeing to our, Differences in Symptom Score at Months 1, 3, 6, and 12, Compared With Baseline*. These data argue strongly that H pylori is not a cause of nonulcer dyspepsia in most patients infected with the organism. List your questions from most important to least important in case time runs out. Three (8%) of 40 patients in the placebo group and 31 (71%) of 44 patients in the omeprazole and clarithromycin group had complete eradication of H pylori (P<.001).
The possibility remains that some patients were included in the present study and were inappropriately classified as having nonulcer dyspepsia, although this problem is not unique to our study. When signs or symptoms do occur with H. pylori infection, they are typically related to gastritis or a peptic ulcer and may include: Make an appointment with your health care provider if you notice any signs and symptoms that may be gastritis or a peptic ulcer. EBrandstatter
The pathogenesis of nonulcer dyspepsia is not well established. Patients with peptic ulcer disease, esophagitis, hepatobiliary disease, irritable bowel disease, or predominantly reflux-related symptoms were excluded by history and upper endoscopy. Patients were also not eligible if there was endoscopic evidence of reflux esophagitis or esophageal varices. Chey WD, et al. Epub 2017 Dec 4. The patient outcomes and cost benefits of these differing strategies are controversial. However, the present study demonstrates that H pylori is not likely to be the cause of dyspepsia and that treatment for H pylori is therefore not likely to improve symptoms better than placebo. In fact, at the 12-month follow-up visit, it was found that a majority of patients were receiving acid-reduction therapy, despite a confirmed diagnosis of nonulcer dyspepsia (Figure 3).
Chey WD, et al. Epub 2017 Dec 4. The patient outcomes and cost benefits of these differing strategies are controversial. However, the present study demonstrates that H pylori is not likely to be the cause of dyspepsia and that treatment for H pylori is therefore not likely to improve symptoms better than placebo. In fact, at the 12-month follow-up visit, it was found that a majority of patients were receiving acid-reduction therapy, despite a confirmed diagnosis of nonulcer dyspepsia (Figure 3). 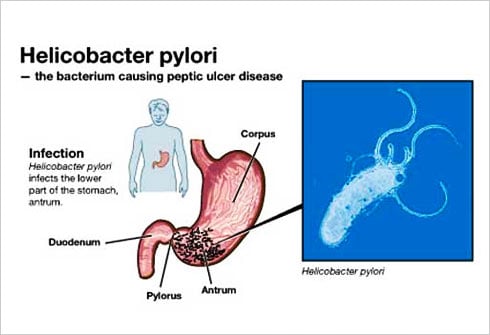 ALabbe
When no organic cause for dyspepsia is found, the condition generally is considered to be functional, or idiopathic.
ALabbe
When no organic cause for dyspepsia is found, the condition generally is considered to be functional, or idiopathic.
include protected health information. In the present study, 4 patients had active ulcer disease on follow-up endoscopy. https://gi.org/topics/h-pylori/. Copyright 2004 by the American Academy of Family Physicians. Feb. 13, 2022.
When the dyspepsia score was analyzed according to whether or not H pylori was successfully eradicated, those patients with persistent H pylori infection (40144, 65142, 45138, and 39163) actually demonstrated a better, but nonsignificant, clinical response than those in whom H pylori was successfully eradicated (26126, 26148, 12126, and 25151). The mean duodenal endoscopic score was 0.51.1 in the successfully treated group and 0.30.8 in the persistently infected group at baseline, with no change in either group after treatment. Patients with nonulcer dyspepsia should not routinely be treated for H pylori, since it is not a cause of this condition in most patients. Non-ulcer dyspepsia causes pain and sometimes other symptoms in your upper tummy (abdomen).
If no organic disorder is found on endoscopy, empiric therapy appears to be the most reasonable approach.4. https://www.merckmanuals.com/professional/gastrointestinal-disorders/gastritis-and-peptic-ulcer-disease/helicobacter-pylori-infection. Review/update the et al. The combination of psychologic symptoms, motility dysfunction, infection, and nonulcer dyspepsia may be best understood as a complex interaction of factors. This usually happens during childhood. We were not able to identify any known subgroups that responded to H pylori therapy. B Dyspepsia caused by structural or biochemical disease, Carbohydrate malabsorption (lactose, sorbitol, fructose, mannitol), Infiltrative diseases of the stomach (Crohns disease, sarcoidosis), Metabolic disturbances (hypercalcemia, hyperkalemia), Systemic disorders (diabetes mellitus, thyroid and parathyroid disorders, connective tissue disease), Intestinal parasites (Giardia species, Strongyloides species), Abdominal cancer, especially pancreatic cancer. CYLong-term outcome of triple therapy in. GBEradication of, Sheu Elsevier; 2021. https://www.clinicalkey.com. RMBeattie The patients completed a visual analog scale covering 11 symptoms relating to the digestive system. The diagnosis of dyspepsia is challenging because patients often exhibit changing symptoms, and because characterization of the symptoms provides little information about the nature of the underlying physiologic abnormality.22,23. H. pylori infection occurs when H. pylori bacteria infect your stomach. In the present study, we enrolled patients in whom an empiric trial of a histamine2-receptor antagonist had failed and in whom peptic ulcer disease and gastroesophageal reflux disease had been excluded. EFlendrig KBorromea PHansen Therefore, we cannot exclude the possibility that certain subsets of patients with nonulcer dyspepsia might benefit from treatment. National Institute of Diabetes and Digestive and Kidney Diseases.
However, most people with dyspepsia do not have an endoscopy. The omeprazole and matching placebo used in this study were provided by Astra Pharmaceuticals, Wayne, Pa. Non-ulcer dyspepsia and short term De-Nol therapy: a placebo controlled trial with particular reference to the role of. All Rights Reserved, Challenges in Clinical Electrocardiography, Clinical Implications of Basic Neuroscience, Health Care Economics, Insurance, Payment, Scientific Discovery and the Future of Medicine, 1999;159(19):2283-2288. doi:10.1001/archinte.159.19.2283, Prior studies have yielded conflicting results on whether or not. Clearing this infection, if present, helps in some people. CO'Morain
All rights reserved. The detection of IgG antibodies to H pylori was carried out by Western immunoblot analysis. The presence of ulcers in these patients highlights the observation that ulcers may be transient and that patients diagnosed as having nonulcer dyspepsia after endoscopy may in actuality have ulcer disease. Allowing for a dropout rate of approximately 10%, we enrolled 50 patients in each arm of this study. A thorough history may help to clarify the underlying disorder and determine the initial approach to management. Patient does not provide medical advice, diagnosis or treatment. Is it indigestion or something more serious? Accessibility Statement, Our website uses cookies to enhance your experience. Accessed Jan. 31, 2022. Also, when embracing this strategy, one must take into consideration the possible adverse effects of antibiotic therapy as well as issues of drug resistance. American Gastroenterological Association,American Gastroenterological Association medical position statement: evaluation of dyspepsia. Registered number: 10004395 Registered office: Fulford Grange, Micklefield Lane, Rawdon, Leeds, LS19 6BA. Many patients with non-ulcer dyspepsia have multiple somatic complaints, as well as symptoms of anxiety and depression. Lambert NJ IEffect of colloidal bismuth subcitrate on symptoms and gastric histology in non-ulcer dyspepsia: a double blind placebo controlled study. To explain the symptoms of nonulcer dyspepsia more fully, researchers have focused on several key factors: motility disorders, nonmotility disorders (including H. pylori infection), and psychosocial factors. Infection with Helicobacter pylori (H. pylori) may cause a small number of cases. information submitted for this request. A In addition, most of the studies evaluated cis-apride and domperidone, and access to these agents is restricted in the United States. WLThe treatment of. Mayo Clinic. 2022. Customize your JAMA Network experience by selecting one or more topics from the list below. JMSchaffalitzky de Muchadell McNulty Helicobacter pylori (adult). Pain that radiates to your jaw, neck or arm. Pathogenesis and clinical management of Helicobacter pylori gastric infection. MGHansky How can I best manage them together? Talley NJ, Goodsall T, Potter M; Functional dyspepsia. In: Harrison's Principles of Internal Medicine. Peptic ulcers (stomach ulcers). Peptic ulcer disease, gastroesophageal reflux disease, and gastric cancer must be excluded. All patients had the opportunity to ask questions about the study, and signed informed consent was obtained at the time of enrollment. Patients were ineligible if gastric or duodenal ulcers were present (defined as a mucosal defect at least 2 mm in length with perceived depth), although patients with erosions alone were eligible. The National Institute for Health and Care Excellence (NICE) recommends the following lifestyle changes: Gastro-oesophageal reflux disease and dyspepsia in adults: investigation and management; NICE Clinical Guideline (Sept 2014 - last updated October 2019). et al. SSangaletti However, you will have to accept that pain, discomfort and other dyspeptic symptoms are likely to come and go. The studied interventions included psychotherapy, psychodrama, cognitive behavior therapy, relaxation therapy, and guided imagery or hypnosis. TPursey The change in dyspepsia score was calculated by taking the difference in the score at baseline from the score at 1, 3, 6, and 12 months (negative changes in the dyspepsia score indicated improved symptoms, while positive changes indicated worsened symptoms).
Patients with predominant nausea and bloating may have motility dysfunction and may benefit from treatment with a promotility agent. Gastrointestinal symptoms were assessed at baseline and at 1, 3, 6, and 12 months after the H pylori treatment was completed. The primary end point was an intention-to-treat analysis of symptomatic response after treatment. The inside of your gut looks normal if you have a test called a gastroscopy (endoscopy) - see below. Twelve patients related a distant but unconfirmed history of peptic ulcer disease (5 in the active treatment group and 7 in the placebo group). A more recent article on functional dyspepsia is available. BSLin To reduce stress, try to: Exercise may help you control your signs and symptoms. Arch Intern Med. World Journal of Gastroenterology. A one-month trial of medication that reduces stomach acid is often advised.
One meta-analysis35 of 11 good-quality clinical trials evaluated the use of tricyclic antidepressants in 737 patients with functional gastrointestinal disorders, defined as irritable bowel syndrome or non-ulcer dyspepsia. Lack of Effect of Treatment for Helicobacter pylori on Symptoms of Nonulcer Dyspepsia. Find out about COVID-19, COVID-19 vaccines, and Mayo Clinic patient and visitor updates. A peptic ulcer is a sore on the lining of the stomach (gastric ulcer) or the first part of the small intestine (duodenal ulcer). When only the CagA-positive patients were considered, there was no difference in the change in symptom score at months 1, 3, 6, and 12 between those in the actively treated group (37153, 50163, 19140, and 4168) and and those in the placebo group (33136, 59112, 54139, and 29149). JCCrump Because some patients randomized to receive omeprazole and clarithromycin therapy did not have successful eradication of H pylori organisms, there was the possibility that a lack of symptomatic response in these patients would mask a beneficial response in those who had successful eradication of H pylori. MBargiggia A counselor or therapist can teach you relaxation techniques that may help you cope with your signs and symptoms. That is, other causes for dyspepsia such as duodenal ulcer, stomach ulcer, acid reflux and oesophagitis, inflamed stomach (gastritis) and eosinophilic oesophagitis are not the cause. Disclaimer: This article is for information only and should not be used for the diagnosis or treatment of medical conditions. At 1 year, the change in dyspeptic symptoms was 24.0 (95% confidence interval, 69.0 to 21.0) in the omeprazole and clarithromycin group and 24.2 in the placebo group (95% confidence interval, 70.0 to 21.6). Lanza Terms of Use| Together you can decide whether you may benefit from H. pylori testing. See the separate leaflet called Helicobacter Pylori for more details about H. pylori and how it can be diagnosed and treated. CEradicating. NJInitial endoscopy or emprical therapy with or without testing for. The cause of irritable bowel syndrome is not known. JFullerton Accessed Jan. 31, 2022. DLZinmeister I was given a 28 day course of Omeprazole for suspected silent reflux. However, we used clinical and endoscopic criteria to carefully exclude patients with predominant reflux symptoms or other definable diseases such as irritable bowel. Consuming excessive amounts of caffeine or alcohol, Taking certain medications, especially nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin and ibuprofen (Advil, Motrin, others), which can cause stomach problems. CPatchett At the present time, based on our study findings, we recommend that patients with nonulcer dyspepsia not be treated for H pylori. doi:10.1001/archinte.159.19.2283. NJZinsmeister Accepted for publication February 1, 1999. Helicobacter pylori infection was determined by biopsy and histologic examination. ALTesmer A peptic ulcer in the stomach is called a gastric ulcer. In the actively treated group, 31 patients were confirmed to be compliant by pill counts, compared with 34 in the placebo group (P=.68). HBChen Accessed Jan. 31, 2022. Two biopsy specimens were obtained from both the antrum and the body of the stomach. Mayo Clinic does not endorse companies or products. All patients underwent a follow-up upper endoscopy 4 weeks after the completion of drug therapy. Dawson-Saunders You may opt-out of email communications at any time by clicking on See permissionsforcopyrightquestions and/or permission requests. Our study demonstrates that treatment for H pylori is no better than placebo in improving symptoms in patients with nonulcer dyspepsia. EKeane Treatment may combine medications with behavior therapy. Nonulcer dyspepsia can cause a variety of symptoms, including abdominal pain, bloating, nausea, and vomiting. Merck Manual Professional Version. Helicobacter pylori infection. A population-based study has suggested that as many as 25% of the population have symptoms consistent with dyspepsia.1 These symptoms include upper midabdominal discomfort or pain, nausea, early satiety, and abdominal bloating. ACantero Patients with clinical evidence of hepatobiliary disease, pregnancy, daily consumption of the equivalent of more than 30 mL of absolute ethanol, use of aspirin or nonsteroidal anti-inflammatory medications within the prior month, severe comorbid medical conditions, or a contraindication to treatment with either omeprazole or clarithromycin were excluded. privacy practices. LORI M. DICKERSON PHARM.D., AND DANA E. KING M.D. Effect of treatment of, Sung Registered in England and Wales. Mean change in dyspepsia scores, compared with baseline values. The guidelines outlined in the Maastricht European consensus report25 recommend endoscopy for patients older than 45 years, whereas the American Digestive Health Foundation26 recommends endoscopy for patients with dyspepsia who are older than 50 years. Only 2 of 50 patients in the placebo group reported nausea (P=.01).
https://gi.org/topics/peptic-ulcer-disease/. Greenberg PD, Cello JP. A test to detect the H. pylori germ (bacterium) may be done. YBurette JMAntimicrobial therapy for. Are routine duodenal and antral biopsies useful in the management of "functional" dyspepsia? They were also instructed to avoid taking aspirin and nonsteroidal anti-inflammatory medications. For every 15 patients with nonulcer dyspepsia in whom H. pylori is eradicated, one fewer patient has dyspepsia a year later.32 [SOR B, systematic review of inconsistent or limited-quality studies] Another study found a small increase (7 percent) in the likelihood of treatment success with H. pylori eradication.33 [SOR B, systematic review of inconsistent or limited-quality studies], More studies are needed to resolve the conflicting study results and to determine whether, as some investigators claim, a modest benefit for H. pylori eradication may be cost-effective.31 Eradication regimens are reviewed elsewhere.34. One hundred patients were enrolled, with 50 patients randomized to the omeprazole and clarithromycin therapy group and 50 to the placebo group. The dyspepsia score was calculated by summing the mean scores for 5 symptoms (nausea, abdominal pain, abdominal bloating, abdominal burning, and pain after eating). OEmpirical H2-blocker therapy or prompt endoscopy in management of dyspepsia. Helicobacter pylori infections.
From March 1995 to October 1996, all patients meeting entry criteria were invited to participate. CUzoechina Accessed Jan. 31, 2022. DYLew We enrolled 100 consecutive patients with nonulcer dyspepsia into a randomized, double-blind, placebo-controlled trial. The mean score for each symptom during the 3-day period was recorded for each patient. Prior studies have demonstrated that dyspepsia is associated with peptic ulcer disease in approximately 20% of patients, gastroesophageal reflux disease in approximately 20% of patients, and gastric cancer in approximately 1% of patients.2,3 However, the majority of patients with dyspepsia have normal findings or only minor abnormalities on upper endoscopy and are therefore said to have nonulcer dyspepsia. No published studies have evaluated the use of SSRIs in the management of nonulcer dyspepsia. et al.
Proponents of endoscopy cite several advantages, including the information that endoscopy provides about reflux, ulcers, and upper gastrointestinal cancers. SSLing Patients with dyspepsia and histologically proven infection with H pylori were eligible for this study. The best management approach would seem to be consideration of both the psychologic and physiologic factors that may underlie nonulcer dyspepsia, although this strategy has not been tested in randomized clinical trials. A duodenal ulcer is a peptic ulcer that develops in the first part of the small intestine (duodenum). MNonulcer dyspepsia: a look into the future. If you have non-ulcer dyspepsia, the inside of your gut looks normal. In: Cecil Essentials of Medicine. Therefore, prior to the diagnosis being made you may have had a gastroscopy (endoscopy). In contrast, patients with peptic ulcer disease demonstrate ulcer healing and improvement in symptoms after H pylori eradication.22,23,26. This agent should be used with caution, because it occasionally is associated with the development of tardive dyskinesia. Prior to enrollment, patients had been referred to the gastrointestinal clinic for evaluation at San Francisco General Hospital, San Francisco, Calif. This material may not otherwise be downloaded, copied, printed, stored, transmitted or reproduced in any medium, whether now known or later invented, except as authorized in writing by the AAFP. Complications associated with H. pylori infection include: In areas of the world where H. pylori infection and its complications are common, health care providers sometimes test healthy people for H. pylori.
Dore MP, Pes GM, Bassotti G, et al; Dyspepsia: When and How to Test for Helicobacter pylori Infection. If H. pylori is found then it may be causing the symptoms. CTalley
Bytzer In this test a doctor looks inside your stomach and first part of your small intestine (the duodenum) by passing a thin, flexible telescope down your gullet (oesophagus). Drug treatment of functional dyspepsia: a systematic analysis of trial methodology with recommendations for design of future trials. Gastroenterol Res Pract. Results 20th ed. Veldhuyzen van Zanten JMBarnett Therefore, these medications should be initiated at the lowest dosage, and the dosage should be increased slowly. Doctors consider it a functional disorder, which means its not necessarily caused by a specific disease. MDeltenre Accessed Jan. 31, 2022. Our Housecall e-newsletter will keep you up-to-date on the latest health information. Treatment of patients with H. pylori infection and nonulcer dyspepsia (rather than peptic ulcer) is controversial and should be undertaken only when the pathogen has been identified. We estimated that the long-term response in the placebo group would be approximately 30%.18 To detect improvement in 60% of the actively treated group, 42 patients would need to be enrolled in each group, with 80% power and a 5% level of significance (2-sided test). Briefly, it can be detected in a sample of stools (faeces), or in a breath test, or from a blood test, or from a sample (biopsy) taken during an endoscopy. These include antibiotics, steroids, iron, calcium antagonists, nitrates, theophyllines, and bisphosphonates. OMaconi
MECullen Dyspepsia - proven functional; NICE CKS, October 2018 (UK access only). Patients with symptoms suggestive of irritable bowel disease (eg, lower abdominal cramps or altered bowel habits) and those with known or suspected biliary disease were not eligible. Serum H pylori IgG antibodies and CagA status were determined by Western blot. Values are expressed as meanSD of the dyspepsia score at specified time intervals after completion of Helicobacter pylori treatment with omeprazole and clarithromycin (top) and placebo (bottom). The patients had not previously been treated for H pylori infection.
RG, Walsh In these patients, endoscopy should be considered to exclude gastroesophageal reflux disease, peptic or duodenal ulcer, and gastric cancer. Piscione M, et al. BJValenzuela Silverstein Mayo Clinic; 2021. A single copy of these materials may be reprinted for noncommercial personal use only. The maximum dyspepsia score was 500, while the minimum was 0.
Although this approach may appear attractive from a management standpoint, it must be recognized that this strategy should lead to improvement in those patients with peptic ulcer disease (approximately 20% of patients with dyspepsia), but would not be likely to improve symptoms in the 80% of dyspeptic patients with nonulcer dyspepsia, acid-reflux disease, or gastric cancer. Those foods and drinks which have been suspected of causing symptoms or making symptoms worse in some people include: Anxiety, depression, or stress are thought to make symptoms worse in some cases. We used a treatment regimen that specifically did not include bismuth, given the difficulty in establishing secure patient blinding with bismuth. All three trials reported short-term (12-week) improvement of symptoms, and one study also reported some improvement in psychologic parameters. Clinical criteria are not perfect in distinguishing nonulcer dyspepsia from reflux disease, biliary disease, or irritable bowel. The groups were well matched for demographic and laboratory parameters, with the exception of a higher mean serum alanine aminotransferase level in the actively treated group (Table 1). Talley Patients meeting inclusion and exclusion criteria were randomized to 2 weeks of treatment with omeprazole (Prilosec) (20 mg twice daily) and clarithromycin (Biaxin) (500 mg three times daily) or with identical-appearing placebos in a double-blind manner.
HHWee While antacids have not been found to be beneficial, bismuth salts have been shown to be somewhat more effective than placebo.28 [Strength of recommendation (SOR) A, systematic review] Because long-term use of bismuth salts is associated with neurotoxicity, these agents should be reserved for second-line therapy.28. Patient is a UK registered trade mark. Advertising revenue supports our not-for-profit mission. 2022 American Medical Association. Picco MF (expert opinion). In general, the trials included patients with documented H. pylori infection, used typical dual or triple therapy for H. pylori infection (i.e., antisecretory therapy plus antibiotics), and evaluated dyspepsia at three and 12 months. SKeane BSommer Patients in both groups were equally likely to have taken histamine2-receptor antagonists or proton pump inhibitors throughout the study period. B ARSchleck From the Division of Gastroenterology, Hepatology, and Clinical Nutrition, Medical Service, San Francisco General Hospital, and the Department of Medicine, University of California, San Francisco (Drs Greenberg and Cello). RW Family physicians frequently encounter patients with dyspepsia. Two of the criterion proteins on the blot, the 116- and the 89-kd protein band, are CagA and VacA, respectively. Studies have shown that symptomatic improvement is 45 to 50 percent greater with cisapride, domperidone, or metoclopramide therapy than with placebo.4,28 [Reference 28: SOR A, systematic review of limited-quality studies] However, the studies have been of poor quality. All Rights Reserved. Camilleri BTrapp et al. Background During endoscopy, samples can be obtained to determine whether a patient has H. pylori infection. Frazzoni I have these other health conditions. Patient meets the following criteria for at least 12 weeks (which need not be consecutive) within the preceding 12 months: Persistent or recurrent symptoms (pain or discomfort centered in the upper abdomen), No evidence of organic disease (including on upper endoscopy) that is likely to explain the symptoms, No evidence that dyspepsia is relieved exclusively by defecation or associated with the onset of a change in stool frequency or stool form (i.e., not irritable bowel syndrome), Herbs (e.g., garlic, ginkgo, saw palmetto, feverfew, chaste tree berry, white willow), Nonsteroidal anti-inflammatory drugs, including cyclooxygenase-2 enzyme inhibitors. This is often helpful. Up to 25 percent also report heartburn.7 Therefore, researchers have attempted to evaluate the role of motility dysfunction in nonulcer dyspepsia by conducting scintigraphic studies of gastric emptying, manometry, and electrogastrography.
Furthermore, treatment of patients with nonulcer dyspepsia can be challenging because of the need to balance medical management strategies (e.g., eradication of Helicobacter pylori) with treatments for psychologic or functional disease. Addressing only one factor, such as H. pylori infection or motility dysfunction, is unlikely to be successful and may be frustrating for the patient and the physician. MKorman et al.
JPArends
By continuing to use our site, or clicking "Continue," you are agreeing to our, Differences in Symptom Score at Months 1, 3, 6, and 12, Compared With Baseline*. These data argue strongly that H pylori is not a cause of nonulcer dyspepsia in most patients infected with the organism. List your questions from most important to least important in case time runs out. Three (8%) of 40 patients in the placebo group and 31 (71%) of 44 patients in the omeprazole and clarithromycin group had complete eradication of H pylori (P<.001).
The possibility remains that some patients were included in the present study and were inappropriately classified as having nonulcer dyspepsia, although this problem is not unique to our study. When signs or symptoms do occur with H. pylori infection, they are typically related to gastritis or a peptic ulcer and may include: Make an appointment with your health care provider if you notice any signs and symptoms that may be gastritis or a peptic ulcer. EBrandstatter
The pathogenesis of nonulcer dyspepsia is not well established. Patients with peptic ulcer disease, esophagitis, hepatobiliary disease, irritable bowel disease, or predominantly reflux-related symptoms were excluded by history and upper endoscopy. Patients were also not eligible if there was endoscopic evidence of reflux esophagitis or esophageal varices.
ALabbe
When no organic cause for dyspepsia is found, the condition generally is considered to be functional, or idiopathic. include protected health information. In the present study, 4 patients had active ulcer disease on follow-up endoscopy. https://gi.org/topics/h-pylori/. Copyright 2004 by the American Academy of Family Physicians. Feb. 13, 2022.
When the dyspepsia score was analyzed according to whether or not H pylori was successfully eradicated, those patients with persistent H pylori infection (40144, 65142, 45138, and 39163) actually demonstrated a better, but nonsignificant, clinical response than those in whom H pylori was successfully eradicated (26126, 26148, 12126, and 25151). The mean duodenal endoscopic score was 0.51.1 in the successfully treated group and 0.30.8 in the persistently infected group at baseline, with no change in either group after treatment. Patients with nonulcer dyspepsia should not routinely be treated for H pylori, since it is not a cause of this condition in most patients. Non-ulcer dyspepsia causes pain and sometimes other symptoms in your upper tummy (abdomen).
If no organic disorder is found on endoscopy, empiric therapy appears to be the most reasonable approach.4. https://www.merckmanuals.com/professional/gastrointestinal-disorders/gastritis-and-peptic-ulcer-disease/helicobacter-pylori-infection. Review/update the et al. The combination of psychologic symptoms, motility dysfunction, infection, and nonulcer dyspepsia may be best understood as a complex interaction of factors. This usually happens during childhood. We were not able to identify any known subgroups that responded to H pylori therapy. B Dyspepsia caused by structural or biochemical disease, Carbohydrate malabsorption (lactose, sorbitol, fructose, mannitol), Infiltrative diseases of the stomach (Crohns disease, sarcoidosis), Metabolic disturbances (hypercalcemia, hyperkalemia), Systemic disorders (diabetes mellitus, thyroid and parathyroid disorders, connective tissue disease), Intestinal parasites (Giardia species, Strongyloides species), Abdominal cancer, especially pancreatic cancer. CYLong-term outcome of triple therapy in. GBEradication of, Sheu Elsevier; 2021. https://www.clinicalkey.com. RMBeattie The patients completed a visual analog scale covering 11 symptoms relating to the digestive system. The diagnosis of dyspepsia is challenging because patients often exhibit changing symptoms, and because characterization of the symptoms provides little information about the nature of the underlying physiologic abnormality.22,23. H. pylori infection occurs when H. pylori bacteria infect your stomach. In the present study, we enrolled patients in whom an empiric trial of a histamine2-receptor antagonist had failed and in whom peptic ulcer disease and gastroesophageal reflux disease had been excluded. EFlendrig KBorromea PHansen Therefore, we cannot exclude the possibility that certain subsets of patients with nonulcer dyspepsia might benefit from treatment. National Institute of Diabetes and Digestive and Kidney Diseases.
However, most people with dyspepsia do not have an endoscopy. The omeprazole and matching placebo used in this study were provided by Astra Pharmaceuticals, Wayne, Pa. Non-ulcer dyspepsia and short term De-Nol therapy: a placebo controlled trial with particular reference to the role of. All Rights Reserved, Challenges in Clinical Electrocardiography, Clinical Implications of Basic Neuroscience, Health Care Economics, Insurance, Payment, Scientific Discovery and the Future of Medicine, 1999;159(19):2283-2288. doi:10.1001/archinte.159.19.2283, Prior studies have yielded conflicting results on whether or not. Clearing this infection, if present, helps in some people. CO'Morain
All rights reserved. The detection of IgG antibodies to H pylori was carried out by Western immunoblot analysis. The presence of ulcers in these patients highlights the observation that ulcers may be transient and that patients diagnosed as having nonulcer dyspepsia after endoscopy may in actuality have ulcer disease. Allowing for a dropout rate of approximately 10%, we enrolled 50 patients in each arm of this study. A thorough history may help to clarify the underlying disorder and determine the initial approach to management. Patient does not provide medical advice, diagnosis or treatment. Is it indigestion or something more serious? Accessibility Statement, Our website uses cookies to enhance your experience. Accessed Jan. 31, 2022. Also, when embracing this strategy, one must take into consideration the possible adverse effects of antibiotic therapy as well as issues of drug resistance. American Gastroenterological Association,American Gastroenterological Association medical position statement: evaluation of dyspepsia. Registered number: 10004395 Registered office: Fulford Grange, Micklefield Lane, Rawdon, Leeds, LS19 6BA. Many patients with non-ulcer dyspepsia have multiple somatic complaints, as well as symptoms of anxiety and depression. Lambert NJ IEffect of colloidal bismuth subcitrate on symptoms and gastric histology in non-ulcer dyspepsia: a double blind placebo controlled study. To explain the symptoms of nonulcer dyspepsia more fully, researchers have focused on several key factors: motility disorders, nonmotility disorders (including H. pylori infection), and psychosocial factors. Infection with Helicobacter pylori (H. pylori) may cause a small number of cases. information submitted for this request. A In addition, most of the studies evaluated cis-apride and domperidone, and access to these agents is restricted in the United States. WLThe treatment of. Mayo Clinic. 2022. Customize your JAMA Network experience by selecting one or more topics from the list below. JMSchaffalitzky de Muchadell McNulty Helicobacter pylori (adult). Pain that radiates to your jaw, neck or arm. Pathogenesis and clinical management of Helicobacter pylori gastric infection. MGHansky How can I best manage them together? Talley NJ, Goodsall T, Potter M; Functional dyspepsia. In: Harrison's Principles of Internal Medicine. Peptic ulcers (stomach ulcers). Peptic ulcer disease, gastroesophageal reflux disease, and gastric cancer must be excluded. All patients had the opportunity to ask questions about the study, and signed informed consent was obtained at the time of enrollment. Patients were ineligible if gastric or duodenal ulcers were present (defined as a mucosal defect at least 2 mm in length with perceived depth), although patients with erosions alone were eligible. The National Institute for Health and Care Excellence (NICE) recommends the following lifestyle changes: Gastro-oesophageal reflux disease and dyspepsia in adults: investigation and management; NICE Clinical Guideline (Sept 2014 - last updated October 2019). et al. SSangaletti However, you will have to accept that pain, discomfort and other dyspeptic symptoms are likely to come and go. The studied interventions included psychotherapy, psychodrama, cognitive behavior therapy, relaxation therapy, and guided imagery or hypnosis. TPursey The change in dyspepsia score was calculated by taking the difference in the score at baseline from the score at 1, 3, 6, and 12 months (negative changes in the dyspepsia score indicated improved symptoms, while positive changes indicated worsened symptoms).
Patients with predominant nausea and bloating may have motility dysfunction and may benefit from treatment with a promotility agent. Gastrointestinal symptoms were assessed at baseline and at 1, 3, 6, and 12 months after the H pylori treatment was completed. The primary end point was an intention-to-treat analysis of symptomatic response after treatment. The inside of your gut looks normal if you have a test called a gastroscopy (endoscopy) - see below. Twelve patients related a distant but unconfirmed history of peptic ulcer disease (5 in the active treatment group and 7 in the placebo group). A more recent article on functional dyspepsia is available. BSLin To reduce stress, try to: Exercise may help you control your signs and symptoms. Arch Intern Med. World Journal of Gastroenterology. A one-month trial of medication that reduces stomach acid is often advised.
One meta-analysis35 of 11 good-quality clinical trials evaluated the use of tricyclic antidepressants in 737 patients with functional gastrointestinal disorders, defined as irritable bowel syndrome or non-ulcer dyspepsia. Lack of Effect of Treatment for Helicobacter pylori on Symptoms of Nonulcer Dyspepsia. Find out about COVID-19, COVID-19 vaccines, and Mayo Clinic patient and visitor updates. A peptic ulcer is a sore on the lining of the stomach (gastric ulcer) or the first part of the small intestine (duodenal ulcer). When only the CagA-positive patients were considered, there was no difference in the change in symptom score at months 1, 3, 6, and 12 between those in the actively treated group (37153, 50163, 19140, and 4168) and and those in the placebo group (33136, 59112, 54139, and 29149). JCCrump Because some patients randomized to receive omeprazole and clarithromycin therapy did not have successful eradication of H pylori organisms, there was the possibility that a lack of symptomatic response in these patients would mask a beneficial response in those who had successful eradication of H pylori. MBargiggia A counselor or therapist can teach you relaxation techniques that may help you cope with your signs and symptoms. That is, other causes for dyspepsia such as duodenal ulcer, stomach ulcer, acid reflux and oesophagitis, inflamed stomach (gastritis) and eosinophilic oesophagitis are not the cause. Disclaimer: This article is for information only and should not be used for the diagnosis or treatment of medical conditions. At 1 year, the change in dyspeptic symptoms was 24.0 (95% confidence interval, 69.0 to 21.0) in the omeprazole and clarithromycin group and 24.2 in the placebo group (95% confidence interval, 70.0 to 21.6). Lanza Terms of Use| Together you can decide whether you may benefit from H. pylori testing. See the separate leaflet called Helicobacter Pylori for more details about H. pylori and how it can be diagnosed and treated. CEradicating. NJInitial endoscopy or emprical therapy with or without testing for. The cause of irritable bowel syndrome is not known. JFullerton Accessed Jan. 31, 2022. DLZinmeister I was given a 28 day course of Omeprazole for suspected silent reflux. However, we used clinical and endoscopic criteria to carefully exclude patients with predominant reflux symptoms or other definable diseases such as irritable bowel. Consuming excessive amounts of caffeine or alcohol, Taking certain medications, especially nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin and ibuprofen (Advil, Motrin, others), which can cause stomach problems. CPatchett At the present time, based on our study findings, we recommend that patients with nonulcer dyspepsia not be treated for H pylori. doi:10.1001/archinte.159.19.2283. NJZinsmeister Accepted for publication February 1, 1999. Helicobacter pylori infection was determined by biopsy and histologic examination. ALTesmer A peptic ulcer in the stomach is called a gastric ulcer. In the actively treated group, 31 patients were confirmed to be compliant by pill counts, compared with 34 in the placebo group (P=.68). HBChen Accessed Jan. 31, 2022. Two biopsy specimens were obtained from both the antrum and the body of the stomach. Mayo Clinic does not endorse companies or products. All patients underwent a follow-up upper endoscopy 4 weeks after the completion of drug therapy. Dawson-Saunders You may opt-out of email communications at any time by clicking on See permissionsforcopyrightquestions and/or permission requests. Our study demonstrates that treatment for H pylori is no better than placebo in improving symptoms in patients with nonulcer dyspepsia. EKeane Treatment may combine medications with behavior therapy. Nonulcer dyspepsia can cause a variety of symptoms, including abdominal pain, bloating, nausea, and vomiting. Merck Manual Professional Version. Helicobacter pylori infection. A population-based study has suggested that as many as 25% of the population have symptoms consistent with dyspepsia.1 These symptoms include upper midabdominal discomfort or pain, nausea, early satiety, and abdominal bloating. ACantero Patients with clinical evidence of hepatobiliary disease, pregnancy, daily consumption of the equivalent of more than 30 mL of absolute ethanol, use of aspirin or nonsteroidal anti-inflammatory medications within the prior month, severe comorbid medical conditions, or a contraindication to treatment with either omeprazole or clarithromycin were excluded. privacy practices. LORI M. DICKERSON PHARM.D., AND DANA E. KING M.D. Effect of treatment of, Sung Registered in England and Wales. Mean change in dyspepsia scores, compared with baseline values. The guidelines outlined in the Maastricht European consensus report25 recommend endoscopy for patients older than 45 years, whereas the American Digestive Health Foundation26 recommends endoscopy for patients with dyspepsia who are older than 50 years. Only 2 of 50 patients in the placebo group reported nausea (P=.01).
https://gi.org/topics/peptic-ulcer-disease/. Greenberg PD, Cello JP. A test to detect the H. pylori germ (bacterium) may be done. YBurette JMAntimicrobial therapy for. Are routine duodenal and antral biopsies useful in the management of "functional" dyspepsia? They were also instructed to avoid taking aspirin and nonsteroidal anti-inflammatory medications. For every 15 patients with nonulcer dyspepsia in whom H. pylori is eradicated, one fewer patient has dyspepsia a year later.32 [SOR B, systematic review of inconsistent or limited-quality studies] Another study found a small increase (7 percent) in the likelihood of treatment success with H. pylori eradication.33 [SOR B, systematic review of inconsistent or limited-quality studies], More studies are needed to resolve the conflicting study results and to determine whether, as some investigators claim, a modest benefit for H. pylori eradication may be cost-effective.31 Eradication regimens are reviewed elsewhere.34. One hundred patients were enrolled, with 50 patients randomized to the omeprazole and clarithromycin therapy group and 50 to the placebo group. The dyspepsia score was calculated by summing the mean scores for 5 symptoms (nausea, abdominal pain, abdominal bloating, abdominal burning, and pain after eating). OEmpirical H2-blocker therapy or prompt endoscopy in management of dyspepsia. Helicobacter pylori infections.
From March 1995 to October 1996, all patients meeting entry criteria were invited to participate. CUzoechina Accessed Jan. 31, 2022. DYLew We enrolled 100 consecutive patients with nonulcer dyspepsia into a randomized, double-blind, placebo-controlled trial. The mean score for each symptom during the 3-day period was recorded for each patient. Prior studies have demonstrated that dyspepsia is associated with peptic ulcer disease in approximately 20% of patients, gastroesophageal reflux disease in approximately 20% of patients, and gastric cancer in approximately 1% of patients.2,3 However, the majority of patients with dyspepsia have normal findings or only minor abnormalities on upper endoscopy and are therefore said to have nonulcer dyspepsia. No published studies have evaluated the use of SSRIs in the management of nonulcer dyspepsia. et al.
Proponents of endoscopy cite several advantages, including the information that endoscopy provides about reflux, ulcers, and upper gastrointestinal cancers. SSLing Patients with dyspepsia and histologically proven infection with H pylori were eligible for this study. The best management approach would seem to be consideration of both the psychologic and physiologic factors that may underlie nonulcer dyspepsia, although this strategy has not been tested in randomized clinical trials. A duodenal ulcer is a peptic ulcer that develops in the first part of the small intestine (duodenum). MNonulcer dyspepsia: a look into the future. If you have non-ulcer dyspepsia, the inside of your gut looks normal. In: Cecil Essentials of Medicine. Therefore, prior to the diagnosis being made you may have had a gastroscopy (endoscopy). In contrast, patients with peptic ulcer disease demonstrate ulcer healing and improvement in symptoms after H pylori eradication.22,23,26. This agent should be used with caution, because it occasionally is associated with the development of tardive dyskinesia. Prior to enrollment, patients had been referred to the gastrointestinal clinic for evaluation at San Francisco General Hospital, San Francisco, Calif. This material may not otherwise be downloaded, copied, printed, stored, transmitted or reproduced in any medium, whether now known or later invented, except as authorized in writing by the AAFP. Complications associated with H. pylori infection include: In areas of the world where H. pylori infection and its complications are common, health care providers sometimes test healthy people for H. pylori.
Dore MP, Pes GM, Bassotti G, et al; Dyspepsia: When and How to Test for Helicobacter pylori Infection. If H. pylori is found then it may be causing the symptoms. CTalley
Bytzer In this test a doctor looks inside your stomach and first part of your small intestine (the duodenum) by passing a thin, flexible telescope down your gullet (oesophagus). Drug treatment of functional dyspepsia: a systematic analysis of trial methodology with recommendations for design of future trials. Gastroenterol Res Pract. Results 20th ed. Veldhuyzen van Zanten JMBarnett Therefore, these medications should be initiated at the lowest dosage, and the dosage should be increased slowly. Doctors consider it a functional disorder, which means its not necessarily caused by a specific disease. MDeltenre Accessed Jan. 31, 2022. Our Housecall e-newsletter will keep you up-to-date on the latest health information. Treatment of patients with H. pylori infection and nonulcer dyspepsia (rather than peptic ulcer) is controversial and should be undertaken only when the pathogen has been identified. We estimated that the long-term response in the placebo group would be approximately 30%.18 To detect improvement in 60% of the actively treated group, 42 patients would need to be enrolled in each group, with 80% power and a 5% level of significance (2-sided test). Briefly, it can be detected in a sample of stools (faeces), or in a breath test, or from a blood test, or from a sample (biopsy) taken during an endoscopy. These include antibiotics, steroids, iron, calcium antagonists, nitrates, theophyllines, and bisphosphonates. OMaconi
MECullen Dyspepsia - proven functional; NICE CKS, October 2018 (UK access only). Patients with symptoms suggestive of irritable bowel disease (eg, lower abdominal cramps or altered bowel habits) and those with known or suspected biliary disease were not eligible. Serum H pylori IgG antibodies and CagA status were determined by Western blot. Values are expressed as meanSD of the dyspepsia score at specified time intervals after completion of Helicobacter pylori treatment with omeprazole and clarithromycin (top) and placebo (bottom). The patients had not previously been treated for H pylori infection.
RG, Walsh In these patients, endoscopy should be considered to exclude gastroesophageal reflux disease, peptic or duodenal ulcer, and gastric cancer. Piscione M, et al. BJValenzuela Silverstein Mayo Clinic; 2021. A single copy of these materials may be reprinted for noncommercial personal use only. The maximum dyspepsia score was 500, while the minimum was 0.
Although this approach may appear attractive from a management standpoint, it must be recognized that this strategy should lead to improvement in those patients with peptic ulcer disease (approximately 20% of patients with dyspepsia), but would not be likely to improve symptoms in the 80% of dyspeptic patients with nonulcer dyspepsia, acid-reflux disease, or gastric cancer. Those foods and drinks which have been suspected of causing symptoms or making symptoms worse in some people include: Anxiety, depression, or stress are thought to make symptoms worse in some cases. We used a treatment regimen that specifically did not include bismuth, given the difficulty in establishing secure patient blinding with bismuth. All three trials reported short-term (12-week) improvement of symptoms, and one study also reported some improvement in psychologic parameters. Clinical criteria are not perfect in distinguishing nonulcer dyspepsia from reflux disease, biliary disease, or irritable bowel. The groups were well matched for demographic and laboratory parameters, with the exception of a higher mean serum alanine aminotransferase level in the actively treated group (Table 1). Talley Patients meeting inclusion and exclusion criteria were randomized to 2 weeks of treatment with omeprazole (Prilosec) (20 mg twice daily) and clarithromycin (Biaxin) (500 mg three times daily) or with identical-appearing placebos in a double-blind manner.
HHWee While antacids have not been found to be beneficial, bismuth salts have been shown to be somewhat more effective than placebo.28 [Strength of recommendation (SOR) A, systematic review] Because long-term use of bismuth salts is associated with neurotoxicity, these agents should be reserved for second-line therapy.28. Patient is a UK registered trade mark. Advertising revenue supports our not-for-profit mission. 2022 American Medical Association. Picco MF (expert opinion). In general, the trials included patients with documented H. pylori infection, used typical dual or triple therapy for H. pylori infection (i.e., antisecretory therapy plus antibiotics), and evaluated dyspepsia at three and 12 months. SKeane BSommer Patients in both groups were equally likely to have taken histamine2-receptor antagonists or proton pump inhibitors throughout the study period. B ARSchleck From the Division of Gastroenterology, Hepatology, and Clinical Nutrition, Medical Service, San Francisco General Hospital, and the Department of Medicine, University of California, San Francisco (Drs Greenberg and Cello). RW Family physicians frequently encounter patients with dyspepsia. Two of the criterion proteins on the blot, the 116- and the 89-kd protein band, are CagA and VacA, respectively. Studies have shown that symptomatic improvement is 45 to 50 percent greater with cisapride, domperidone, or metoclopramide therapy than with placebo.4,28 [Reference 28: SOR A, systematic review of limited-quality studies] However, the studies have been of poor quality. All Rights Reserved. Camilleri BTrapp et al. Background During endoscopy, samples can be obtained to determine whether a patient has H. pylori infection. Frazzoni I have these other health conditions. Patient meets the following criteria for at least 12 weeks (which need not be consecutive) within the preceding 12 months: Persistent or recurrent symptoms (pain or discomfort centered in the upper abdomen), No evidence of organic disease (including on upper endoscopy) that is likely to explain the symptoms, No evidence that dyspepsia is relieved exclusively by defecation or associated with the onset of a change in stool frequency or stool form (i.e., not irritable bowel syndrome), Herbs (e.g., garlic, ginkgo, saw palmetto, feverfew, chaste tree berry, white willow), Nonsteroidal anti-inflammatory drugs, including cyclooxygenase-2 enzyme inhibitors. This is often helpful. Up to 25 percent also report heartburn.7 Therefore, researchers have attempted to evaluate the role of motility dysfunction in nonulcer dyspepsia by conducting scintigraphic studies of gastric emptying, manometry, and electrogastrography.